

Background
Despite prophylaxis, GVHD remains a significant cause of morbidity and nonrelapse mortality after allogeneic hematopoietic cell transplantation (HCT). ITA is a potent, selective Janus kinase (JAK) 1 inhibitor that has been combined safely with steroids in patients (pts) with acute GVHD. We describe results from a proof-of-concept study evaluating ITA + CNI-based regimens for GVHD prophylaxis.
Study Design and Methods
GRAVITAS-119 (NCT03320642) was a single-arm, open-label study enrolling pts aged ≥18 y undergoing allogeneic HCT using peripheral blood stem cells from 8/8 or 7/8 matched related or unrelated donors for a hematologic malignancy. Eligible pts were candidates for reduced-intensity conditioning with Karnofsky Performance Status ≥70%. Pts were excluded for prior HCT, JAK inhibitor therapy, or active uncontrolled infection. Pts received oral ITA 200 mg once daily (QD) beginning 3 d before HCT + tacrolimus (Tac)/methotrexate (MTX) or cyclosporine A (CSA)/mycophenolate mofetil (MMF) ± antithymocyte globulin (ATG) per institutional practice. ITA dose reduction/interruption was permitted for toxicity. ITA was reduced to 100 mg QD by Day 90 and discontinued by Day 180 unless pts required systemic GVHD treatment (tx), had malignancy relapse or unacceptable toxicity, or withdrew consent. The primary endpoint was Day 28 hematologic recovery (absolute neutrophil count [ANC] ≥500/mm3 for 3 consecutive measurements and platelets [plt] ≥20,000/mm3 with no transfusions in the preceding 3 d). Secondary endpoints included incidence of acute and chronic GVHD, GVHD- and relapse-free survival (GRFS), overall survival, and safety.
Results
Sixty-five pts were enrolled and treated with ITA + Tac/MTX (n=41; +ATG, n=8; no ATG, n=33) or ITA + CSA/MMF (n=24; +ATG, n=16; no ATG, n=8). Median (range) age was 65 (25-76) y, and 57% were male. The most common underlying malignancies were acute myeloid leukemia (40%) and myelodysplastic syndrome (26%). Disease risk index was classified as low, intermediate, and high in 11%, 66%, and 23% of pts, respectively. Pts received grafts from matched related (51%), matched unrelated (40%), or single-antigen mismatched unrelated (9%) donors. Busulfan/fludarabine (51%) and a fludarabine/melphalan reduced-intensity regimen (18%) were the most common conditioning regimens; 11% of regimens contained total body irradiation.
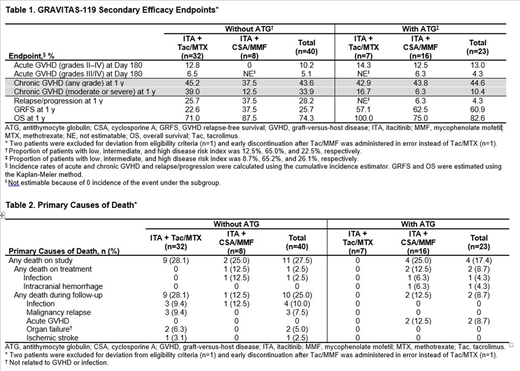
Median (range) exposure to ITA was 140 (10-187) d; 74% received ITA for >90 d. All pts achieved hematologic recovery. Median (range) time to ANC and plt recovery among patients who had count nadir (ANC <500/mm3 and/or plt <20,000/mm3) was 17 (4-31) and 14 (9-26) d, respectively. ANC recovery was on Day 31 for 1 pt with secondary myelofibrosis (MF). Two pts had secondary graft failure, 1 on tx (Tac/MTX/ATG; Day 65), with no evidence of viral infection, and 1 during post-tx follow-up (Tac/MTX; Day 182); both underwent retransplantation. Malignancy relapse (median follow-up, 363 d) occurred in 12 pts (18%), including 3 pts with molecular/cytogenetic relapse requiring intervention. In 63 evaluable pts, cumulative incidence of grade III/IV acute GVHD at Day 180 was 4.8% and 1-y GRFS was 38.5%. Secondary efficacy endpoints by tx group are in Table 1. The most common grade 3/4 hematologic adverse events (AEs) were thrombocytopenia (49%) and anemia (31%). 17 pts (26%) had cytomegalovirus reactivations (n=10 +ATG), 8 (12%) had Epstein-Barr virus (EBV) infection (no post-transplant lymphoproliferative disorder cases; all +ATG), and 1 pt (2%) had invasive bronchopulmonary aspergillosis (Tac/MTX +ATG). AEs (22%) and relapse (17%) were the most common reasons for ITA discontinuation; the most common AEs leading to discontinuation were mixed chimerism (6%), thrombocytopenia (3%), and hypertriglyceridemia (3%). 8 pts in the +ATG group received post-transplant rituximab for EBV infection (n=7) and/or azaciditine maintenance therapy (n=3). 15 pts (24%) in the per-protocol population died. 3 deaths occurred on tx due to infections (n=2) and intracranial hemorrhage (n=1; Table 2).
Conclusions
Results from this small open-label trial in a heterogeneous pt population demonstrated that GVHD prophylaxis with ITA + CNI-based regimens was well tolerated and rates of severe acute GVHD were low. 1 pt with MF did not achieve ANC recovery on Day 28. An ITA + Tac + post-transplant cyclophosphamide cohort is currently being investigated in GRAVITAS-119.
Shah:Cell Vault: Research Funding; Celgene: Consultancy, Honoraria; Miltenyi Biotec: Honoraria, Research Funding; Kite Pharma: Consultancy, Honoraria; Incyte: Consultancy; TG Therapeutics: Consultancy; Verastim: Consultancy; Lily: Consultancy, Honoraria. Chevallier:Incyte Corporation: Honoraria. Rubio:Medac: Consultancy; MSD: Honoraria; Gilead: Honoraria; Neovii: Research Funding; Novartis: Honoraria. Schroeder:Astellas: Other; Dova Pharmaceuticals: Other; FlatIron Inc: Other; GSK: Other; Gilead Sciences Inc: Other; Novo Nordisk: Other; Genentech Inc: Research Funding; Merck: Consultancy, Honoraria, Speakers Bureau; Takeda: Consultancy, Honoraria, Speakers Bureau; Incyte Corporation: Other: served on advisory boards and received honoraria or consultant fees, Research Funding; Cellect Inc: Research Funding; Janssen: Research Funding; Partners Therapeutics: Other; Pfizer: Other; AbbVie: Consultancy, Honoraria, Speakers Bureau; Fortis: Research Funding; Seattle Genetics: Research Funding; Amgen: Other: served on advisory boards and received honoraria or consultant fees, Research Funding; Celgene: Research Funding; PBD Incorporated: Research Funding; Genzyme Sanofi: Other: served on advisory boards and received honoraria or consultant fees, Research Funding. Hardy:Incyte Corporation: Other: Advisory Board Member; Kite/Gilead: Other: Advisory Board Member; American Gene Technologies: Other: DSMB Member. Stiff:Kite, a Gilead Company: Research Funding; Amgen: Research Funding; Gamida Cell: Research Funding; Atara: Research Funding; Unum: Research Funding; Delta-Fly: Research Funding; Macrogenics: Research Funding. Solano:Incyte Corporation: Other: Received fees for an advisory role. Yakoub-Agha:Celgene: Honoraria; Novartis: Honoraria; Gilead/Kite: Honoraria, Other: travel support; Janssen: Honoraria; Jazz Pharmaceuticals: Honoraria. Rowley:AbbVie: Current equity holder in publicly-traded company; FATE Therapeutics: Consultancy. Duarte:Incyte Corporation: Other: Has received speaker and advisor fees. Morariu-Zamfir:Incyte Corporation: Current Employment, Current equity holder in publicly-traded company. Arbushites:Incyte Corporation: Current Employment, Current equity holder in publicly-traded company. Ding:Incyte Corporation: Current Employment, Current equity holder in publicly-traded company. Perales:Miltenyi Biotec: Research Funding; Kite/Gilead: Honoraria, Research Funding; Incyte Corporation: Honoraria, Research Funding; Nektar Therapeutics: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; Cidara Therapeutics: Other; Servier: Membership on an entity's Board of Directors or advisory committees, Other; NexImmune: Membership on an entity's Board of Directors or advisory committees; Medigene: Membership on an entity's Board of Directors or advisory committees, Other; Omeros: Honoraria, Membership on an entity's Board of Directors or advisory committees; MolMed: Membership on an entity's Board of Directors or advisory committees; Bellicum: Honoraria, Membership on an entity's Board of Directors or advisory committees; Abbvie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Merck: Consultancy, Honoraria; Bristol Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Honoraria.
Itacitinib is a novel JAK1 inhibitor that has not been approved for use in acute GVHD or for any other indication.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal